Chengdu is one of the earliest pilot cities for urban-rural basic medical insurance integration in China. This study aimed to analyze the influencing factors of hospitalization costs of senile cataract in a tertiary hospital in Chengdu by robust method, especially considering the influence of medical insurance type. A total of 1310 discharged patients from a tertiary hospital from January 2020 to June 2021 who were mainly diagnosed with senile cataracts were selected as the research subjects. Kruskal-Wallis H test and Spearman correlation analysis are used to conduct univariate statistical analysis. The robust multivariate linear regression model and a semi-parametric multivariate regression model are established to obtain the influencing factors for their hospitalization costs. The robust multivariate regression model results show that reimbursement ratio, number of surgeries, type of medical insurance, hospitalization days, number of additional diagnoses and material proportion have significant correlations with the response variable, i.e. total hospitalization costs of the senile cataract patients. In the robust multivariate regression analysis, the type of insurance is significantly associated with the hospitalization costs. Fixing other variables, the hospitalization costs of patients with UEBMI insurance were 7.6% higher than those with URRBMI insurance. Generalized additive model (GAM) can express the nonlinear relationship between explanatory variables and response variable. Because of the nonlinear part of the GAM, the interpretation and description of the model can provide more knowledge than the linear models. In the GAM model, the type of insurance is also significantly related to the total costs. According to the regression effects of reimbursement ratio, number of surgeries, type of medical insurance, hospitalization days, number of additional diagnoses and material proportion on total costs, the paper aims to provide some references for promoting the reform of the local medical system and improving the eye health status and quality of life of middle-aged and elderly groups.
| Published in | American Journal of Life Sciences (Volume 12, Issue 2) |
| DOI | 10.11648/j.ajls.20241202.12 |
| Page(s) | 33-43 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Senile Cataract, Medical Insurance, Hospitalization Costs, Influencing Factors, Robust Regression, Generalized Additive Model
2.1. The Data Source
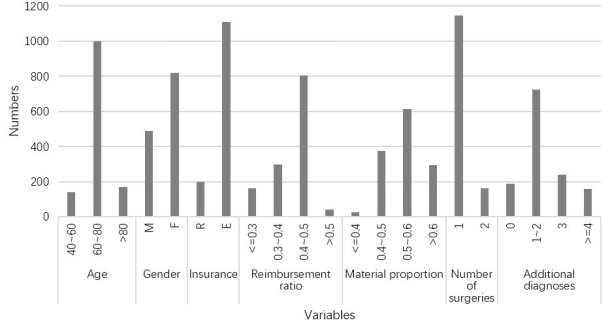
2.2. Descriptive Analysis of Data
Variable | Num | % | total costs (RMB) | ||||
|---|---|---|---|---|---|---|---|
Mean | Sd | Median | P value | ||||
Age | 40~60 | 141 | 0.11 | 10650.40 | 3912.67 | 8419.57 | 0.504 |
60~80 | 998 | 0.76 | 10047.68 | 4922.88 | 8416.95 | ||
>80 | 168 | 0.13 | 10406.69 | 4981.44 | 8563.96 | ||
Gender | M | 489 | 0.37 | 9931.99 | 4884.46 | 8401.26 | 0.522 |
F | 818 | 0.63 | 10294.46 | 5089.54 | 8435.11 | ||
Insurance | R | 199 | 0.15 | 9429.74 | 3765.95 | 8134.07 | 0.005 |
E | 1108 | 0.85 | 10289.80 | 5198.25 | 8461.16 | ||
Reimbursement ratio | <=0.3 | 162 | 0.12 | 17428.88 | 8518.23 | 16795.10 | <0.001 |
0.3~0.4 | 299 | 0.23 | 8168.05 | 2625.60 | 7245.45 | ||
0.4~0.5 | 806 | 0.62 | 9478.75 | 3211.50 | 8491.58 | ||
>0.5 | 40 | 0.03 | 9300.46 | 4105.41 | 8156.40 | ||
Material proportion | <=0.4 | 25 | 0.02 | 12019.54 | 8026.26 | 8792.84 | <0.001 |
0.4~0.5 | 373 | 0.29 | 9687.91 | 3103.14 | 8722.71 | ||
0.5~0.6 | 615 | 0.47 | 9071.33 | 3387.89 | 8315.22 | ||
>0.6 | 294 | 0.22 | 12873.01 | 7752.11 | 9612.35 | ||
Number of surgeries | 1 | 1145 | 0.88 | 8872.86 | 2795.91 | 8257.85 | <0.001 |
2 | 162 | 0.12 | 19248.10 | 7319.70 | 16820.50 | ||
Additional diagnoses | 0 | 189 | 0.15 | 11847.10 | 7221.35 | 8678.72 | <0.001 |
1-2 | 722 | 0.55 | 10157.41 | 4597.19 | 8451.97 | ||
3 | 239 | 0.18 | 9410.62 | 3967.44 | 8232.85 | ||
>=4 | 157 | 0.12 | 9272.14 | 4572.97 | 7865.32 | ||
Variable | materials fee | surgery fee | ||
|---|---|---|---|---|
correlation coefficient | P value | correlation coefficient | P value | |
Age | -0.010 | 0.726 | 0.072 | 0.009 |
Gender | -0.060 | 0.031 | -0.066 | 0.018 |
Hospitalization days | 0.437 | <0.001 | 0.637 | <0.001 |
Reimbursement ratio | -0.353 | <0.001 | 0.026 | 0.346 |
Insurance | 0.087 | 0.002 | 0.034 | 0.217 |
Number of surgeries | 0.467 | <0.001 | 0.830 | <0.001 |
Material proportion | 0.308 | <0.001 | -0.028 | 0.317 |
Additional diagnoses | -0.140 | <0.001 | -0.043 | 0.117 |
2.3. Introduction to Statistical Models
Gender | F→0; M→ 1 |
Insurance | R→0; E→ 1 |
| Log (Hospitalization costs) |
|---|---|
| Age |
| Gender |
| Hospitalization days |
| Reimbursement ratio |
| Insurance |
| Number of surgeries |
| Material proportion |
| Additional diagnoses |
Classical multivariate regression (OLS) | Robust multivariate regression (M-estimation) | |||
|---|---|---|---|---|
Estimator | P value | Estimator | P value | |
Intercept item | 9.440 | <0.001 | 9.675 | <0.001 |
Age | -0.0002 | 0.674 | -0.0004 | 0.548 |
Gender | 0.011 | 0.250 | 0.011 | 0.258 |
Hospitalization days | 0.068 | <0.001 | 0.062 | <0.001 |
Reimbursement ratio | -2.298 | <0.001 | -2.510 | <0.001 |
Insurance | 0.080 | <0.001 | 0.076 | <0.001 |
Number of surgeries | 0.514 | <0.001 | 0.526 | <0.001 |
Material proportion | -0.132 | 0.277 | -0.388 | 0.002 |
Additional diagnoses | -0.022 | <0.001 | -0.022 | <0.001 |
AIC | -970.366 | -921.324 | ||
Sd(res) | 0.167 | 0.169 | ||
MSE | 0.027 | 0.029 | ||
MAE | 0.138 | 0.137 | ||
Parameter estimation of GAM parameter section | ||
|---|---|---|
Variable | Estimator | P value |
Intercept item | 8.361 | <0.001 |
Age | 0.001 | 0.028 |
Gender | -0.002 | 0.699 |
Hospitalization days | 0.036 | <0.001 |
Insurance | 0.037 | <0.001 |
Number of surgeries | 0.580 | <0.001 |
Additional diagnoses | -0.007 | 0.002 |
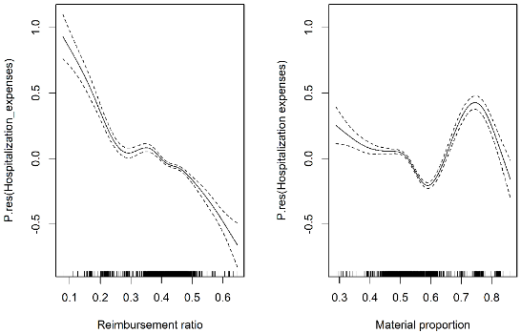
Results of the non-parametric part of GAM | ||
Smooth component | Df | P value |
Reimbursement ratio | 8.311 | <0.001 |
Material proportion | 8.572 | <0.001 |
AIC: -2330.992 | GCV: 0.010 | Sd(res): 0.097 |
MSE: 0.009 | MAE: 0.065 | |
| [1] | Yip WCM, Hsiao WC, Chen W, et al. Early appraisal of China's huge and complex health-care reforms. Lancet. 2012; 379(9818): 833-42. |
| [2] | You XD, Kobayashi Y. The new cooperative medical scheme in China. Health Policy. 2008; 91: 1-9. |
| [3] | Lin W, Liu GG, Chen G. The Urban Resident Basic Medical Insurance: A landmark reform towards universal coverage in China. Health Economics. 2009; 18: S83-S96. |
| [4] | Fan X, Su M, Si Y, et al. The benefits of an integrated social medical insurance for health services utilization in rural China: evidence from the China health and retirement longitudinal study. International Journal for Equity in Health. 2021; 20: 126. |
| [5] | Xue ZX, Li BW. The Impact of the Integration of Urban and Rural Medical Insurance on Migrant Workers' Overwork: Evidence From China. Frontiers in Public Health. 2022; 10: 934524. |
| [6] | Reis T, Lansingh V, Ramke J, et al. Cataract as a Cause of Blindness and Vision Impairment in Latin America: Progress Made and Challenges Beyond 2020. American Journal of Ophthalmology. 2021; 225: 1-10. |
| [7] | To KG, Meuleners LB, Fraser ML, et al. The impact of cataract surgery on vision-related quality of life for bilateral cataract patients in Ho Chi Minh City, Vietnam: a prospective study. Health and Quality of Life Outcomes. 2014; 12: 16. |
| [8] | Khairallah M, Kahloun R, Bourne R, et al. Number of People Blind or Visually Impaired by Cataract Worldwide and in World Regions, 1990 to 2010. Investigative Ophthalmology & Visual Science. 2015; 56(11): 6762-6769. |
| [9] | GBD 2017 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018; 392(10159): 1859-1922. |
| [10] | World Health Organization (2019). World Report on Vision. Available at: |
| [11] | Nangia V, Jonas JB, George R, et al. Prevalence and causes of blindness and vision impairment: magnitude, temporal trends and projections in South and Central Asia. The British Journal of Ophthalmology. 2019; 103(7): 871-877. |
| [12] | Zhu M, Yu J, Zhang J, et al. Evaluating vision-related quality of life in preoperative age-related cataract patients and analyzing its influencing factors in China: a cross-sectional study. BMC Ophthalmology. 2015; 15: 160. |
| [13] | Xiao BX, Yi JL, Limburg H, et al. The prevalence of blindness, visual impairment and cataract surgery in Tuoketuo and Shangdu Counties, Inner Mongolia, China. Open Journal of Ophthalmology. 2015; 5(1): 23-30. |
| [14] | Zheng YF, Huang WY, Xiao BX, et al. Preferences for participation in shared decision-making among cataract patients in urban southern China: a cross-sectional study. Lancet. 2016; 388(1): S56. |
| [15] | Du YF, Liu HR, Zhang Y, et al. Prevalence of cataract and cataract surgery in urban and rural Chinese populations over 50 years old: a systematic review and Meta-analysis. International Journal of Ophthalmology. 2022; 15(1): 141-149. |
| [16] | Yao K and Wang W. A summary of 70 years of cataract diagnosis and treatment in China. Chinese Journal of Ophthalmology. 2020; 56(5): 321-324. |
| [17] | Khan A, Amitava AK, Rizvi SA, et al. Cost-effectiveness analysis should continually assess competing health care options especially in high volume environments like cataract surgery. Indian Journal of Ophthalmology. 2015; 63(6): 496-500. |
| [18] | Deng Y, Yang D, Yu JM, et al. The Association of Socioeconomic Status with the Burden of Cataract-related Blindness and the Effect of Ultraviolet Radiation Exposure: An Ecological Study. Biomedical and Environmental Sciences. 2021; 34(2): 101-109. |
| [19] | Ko F, Frick KD, Tzu J, et al. Willingness to pay for potential enhancements to a low-cost cataract surgical package in rural southern China. Acta Ophthalmologica. 2011; 90: e54-e60. |
| [20] | Tan H, Xie L, Wang Y, et al. Examine the Burden of Illness of US Medicare Patients Diagnosed with Cataract. Value in Health. 2016; 19: A123-A124. |
| [21] | Bhuiyan MU, Luby SP, Alamgir NI, et al. Costs of hospitalization with respiratory syncytial virus illness among children aged <5 years and the financial impact on households in Bangladesh, 2010. Journal of Global Health. 2017; 7(1): 010412. |
| [22] | Luo AJ, Chang WF, Xin ZR, et al. Diagnosis related group grouping study of senile cataract patients based on E-CHAID algorithm. International Journal of Ophthalmology. 2018; 11(2): 308-313. |
| [23] | Xu F, Liu Y, Wheaton AG, et al. Trends and Factors Associated with Hospitalization Costs for Inflammatory Bowel Disease in the United States. Applied Health Economics and Health Policy. 2019; 17(1): 77-91. |
| [24] | Urbich M, Globe G, Pantiri K, et al. A Systematic Review of Medical Costs Associated with Heart Failure in the USA (2014–2020). PharmacoEconomics. 2020; 38(11): 1219-1236. |
| [25] | Rodriguez-Martinez CE, Sossa-Briceño MP, Castro-Rodriguez JA. Direct medical costs of RSV-related bronchiolitis hospitalizations in a middle-income tropical country. Allergologia et Immunopathologia. 2020; 48(1): 56-61. |
| [26] | Gogate PM, Deshpande M and Wormald RP. Is manual small incision cataract surgery affordable in the developing countries? A cost comparison with extracapsular cataract extraction. The British Journal of Ophthalmology. 2003; 87(7): 843-846. |
| [27] | Fu L, Wang Y and Cai F. A working likelihood approach for robust regression. Statistical Methods in Medical Research. 2020; 29(12): 3641-3652. |
| [28] | Yang T, Gallagher C and McMahan CS. A robust regression methodology via M-estimation. Communications in Statistics - Theory and Methods. 2018; 48(5): 1-16. |
| [29] | Huber PJ. Robust Regression: Asymptotics, Conjectures and Monte Carlo. The Annals of Statistics. 1973; 1(5): 799-821. |
| [30] | Hastie T and Tibshirani R. Generalized Additive Models. Statistical Science. 1986; 1(3): 297-318. |
| [31] | Yang J, Zhang M, Chen Y, et al. A study on the relationship between air pollution and pulmonary tuberculosis based on the general additive model in Wulumuqi, China. International Journal of Infectious Diseases. 2020; 96: 42-47. |
| [32] | Dastoorpoor M, Khanjani N, Moradgholi A, et al. Prenatal exposure to ambient air pollution and adverse pregnancy outcomes in Ahvaz, Iran: a generalized additive model. International Archives of Occupational and Environmental Health. 2021; 94(2): 309-324. |
APA Style
Tian, H., Li, T., Lu, S. (2024). Robust Analysis of the Influencing Factors for Hospitalization Costs of Senile Cataracts Patients in Chengdu Considering Different Types of Insurance. American Journal of Life Sciences, 12(2), 33-43. https://doi.org/10.11648/j.ajls.20241202.12
ACS Style
Tian, H.; Li, T.; Lu, S. Robust Analysis of the Influencing Factors for Hospitalization Costs of Senile Cataracts Patients in Chengdu Considering Different Types of Insurance. Am. J. Life Sci. 2024, 12(2), 33-43. doi: 10.11648/j.ajls.20241202.12
AMA Style
Tian H, Li T, Lu S. Robust Analysis of the Influencing Factors for Hospitalization Costs of Senile Cataracts Patients in Chengdu Considering Different Types of Insurance. Am J Life Sci. 2024;12(2):33-43. doi: 10.11648/j.ajls.20241202.12
@article{10.11648/j.ajls.20241202.12,
author = {Haitao Tian and Tianjun Li and Shiqi Lu},
title = {Robust Analysis of the Influencing Factors for Hospitalization Costs of Senile Cataracts Patients in Chengdu Considering Different Types of Insurance
},
journal = {American Journal of Life Sciences},
volume = {12},
number = {2},
pages = {33-43},
doi = {10.11648/j.ajls.20241202.12},
url = {https://doi.org/10.11648/j.ajls.20241202.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajls.20241202.12},
abstract = {Chengdu is one of the earliest pilot cities for urban-rural basic medical insurance integration in China. This study aimed to analyze the influencing factors of hospitalization costs of senile cataract in a tertiary hospital in Chengdu by robust method, especially considering the influence of medical insurance type. A total of 1310 discharged patients from a tertiary hospital from January 2020 to June 2021 who were mainly diagnosed with senile cataracts were selected as the research subjects. Kruskal-Wallis H test and Spearman correlation analysis are used to conduct univariate statistical analysis. The robust multivariate linear regression model and a semi-parametric multivariate regression model are established to obtain the influencing factors for their hospitalization costs. The robust multivariate regression model results show that reimbursement ratio, number of surgeries, type of medical insurance, hospitalization days, number of additional diagnoses and material proportion have significant correlations with the response variable, i.e. total hospitalization costs of the senile cataract patients. In the robust multivariate regression analysis, the type of insurance is significantly associated with the hospitalization costs. Fixing other variables, the hospitalization costs of patients with UEBMI insurance were 7.6% higher than those with URRBMI insurance. Generalized additive model (GAM) can express the nonlinear relationship between explanatory variables and response variable. Because of the nonlinear part of the GAM, the interpretation and description of the model can provide more knowledge than the linear models. In the GAM model, the type of insurance is also significantly related to the total costs. According to the regression effects of reimbursement ratio, number of surgeries, type of medical insurance, hospitalization days, number of additional diagnoses and material proportion on total costs, the paper aims to provide some references for promoting the reform of the local medical system and improving the eye health status and quality of life of middle-aged and elderly groups.
},
year = {2024}
}
TY - JOUR T1 - Robust Analysis of the Influencing Factors for Hospitalization Costs of Senile Cataracts Patients in Chengdu Considering Different Types of Insurance AU - Haitao Tian AU - Tianjun Li AU - Shiqi Lu Y1 - 2024/04/12 PY - 2024 N1 - https://doi.org/10.11648/j.ajls.20241202.12 DO - 10.11648/j.ajls.20241202.12 T2 - American Journal of Life Sciences JF - American Journal of Life Sciences JO - American Journal of Life Sciences SP - 33 EP - 43 PB - Science Publishing Group SN - 2328-5737 UR - https://doi.org/10.11648/j.ajls.20241202.12 AB - Chengdu is one of the earliest pilot cities for urban-rural basic medical insurance integration in China. This study aimed to analyze the influencing factors of hospitalization costs of senile cataract in a tertiary hospital in Chengdu by robust method, especially considering the influence of medical insurance type. A total of 1310 discharged patients from a tertiary hospital from January 2020 to June 2021 who were mainly diagnosed with senile cataracts were selected as the research subjects. Kruskal-Wallis H test and Spearman correlation analysis are used to conduct univariate statistical analysis. The robust multivariate linear regression model and a semi-parametric multivariate regression model are established to obtain the influencing factors for their hospitalization costs. The robust multivariate regression model results show that reimbursement ratio, number of surgeries, type of medical insurance, hospitalization days, number of additional diagnoses and material proportion have significant correlations with the response variable, i.e. total hospitalization costs of the senile cataract patients. In the robust multivariate regression analysis, the type of insurance is significantly associated with the hospitalization costs. Fixing other variables, the hospitalization costs of patients with UEBMI insurance were 7.6% higher than those with URRBMI insurance. Generalized additive model (GAM) can express the nonlinear relationship between explanatory variables and response variable. Because of the nonlinear part of the GAM, the interpretation and description of the model can provide more knowledge than the linear models. In the GAM model, the type of insurance is also significantly related to the total costs. According to the regression effects of reimbursement ratio, number of surgeries, type of medical insurance, hospitalization days, number of additional diagnoses and material proportion on total costs, the paper aims to provide some references for promoting the reform of the local medical system and improving the eye health status and quality of life of middle-aged and elderly groups. VL - 12 IS - 2 ER -
School of Mathematical Sciences, University of Electronic Science and Technology of China, Chengdu, China
Department of Medical Insurance, West China Hospital of Sichuan University, Chengdu, China
Department of Statistics, Southwest Jiaotong University, Chengdu, China